CONSIDERACIONES DE COBERTURA
Factores que influyen en la cobertura
Los terceros pagadores (por ejemplo, aseguradoras comerciales, Medicare, Medicaid) generalmente cubrirán los medicamentos parenterales para sus indicaciones aprobadas por la Administración de Alimentos y Medicamentos de los Estados Unidos (FDA) y los servicios profesionales asociados de administración. Sin embargo, los beneficios pueden variar según el pagador y el plan específico (“producto de seguro”) en el que esté inscrito el paciente.
- NECESIDAD MÉDICA
Cuando los terceros pagadores revisan reclamaciones, primero determinarán si el tipo de servicio proporcionado está cubierto bajo sus políticas. Luego, los pagadores buscarán evidencia que respalde la necesidad médica de la terapia. Esta evidencia puede incluir:
- Información sobre la condición médica y el historial del paciente
- Declaración del médico o Carta de Necesidad Médica
- Literatura de apoyo (por ejemplo, estudios revisados por pares y monografías compendiales)
- Información completa de prescripción
- Disponibilidad de otras alternativas de tratamiento
La necesidad médica se refiere a una decisión de un plan de salud de que un tratamiento, prueba o procedimiento es necesario para la salud o para tratar un problema médico diagnosticado. Las compañías de seguros de salud solo cubren servicios relacionados con la salud que ellos definen o determinan como médicamente necesarios.
Las Determinaciones Nacionales de Cobertura (NCD) de Medicare y las Determinaciones Locales de Cobertura (LCD) de los Contratistas Administrativos de Medicare (MAC) definen los requisitos de necesidad médica para la cobertura de Medicare. Estos documentos contienen orientación sobre diagnósticos cubiertos, documentación requerida y limitaciones de cobertura para servicios específicos de acuerdo con la necesidad médica.
- CONSIDERACIONES ADMINISTRATIVAS
Otras consideraciones pueden influir en la decisión de un pagador de cubrir un producto o servicio:
- ¿El contrato del pagador indica específicamente los lugares de atención que pueden facturar servicios de infusión o medicamentos administrados por infusión? Una pequeña porción de los pagadores tiene contratos exclusivos con proveedores preferidos designados para servicios de infusión. Esto puede incluir ciertas clínicas o farmacias especializadas que entregan medicamentos a proveedores de atención médica u otros centros de infusión.
- ¿El pagador cubre la terapia solo cuando se proporciona en un sitio de tratamiento específico? Los pagadores pueden tener reglas de cobertura específicas por sitio que restringen la provisión de terapias infundidas. Por ejemplo, actualmente Medicare no cubre infusiones cuando son facturadas por centros de cirugía ambulatoria certificados por Medicare. Los pagadores también pueden restringir la cobertura de ciertos medicamentos infundidos en el hogar o en el entorno ambulatorio hospitalario.
- ¿El proveedor de facturación es un miembro “participante” o un proveedor “dentro de la red” para ese plan en particular? Los pagadores contratan con proveedores para ofrecer servicios a los miembros del plan. Por lo tanto, los proveedores son “participantes” o están dentro de la red de ese plan, lo que requiere que cumplan con la estructura de cargos del contrato al proporcionar atención a los miembros de ese plan.
- ¿Está dispuesto el plan a otorgar el estatus de dentro de la red cuando un servicio está fuera de la red? En algunos casos (por ejemplo, cuando no hay proveedores disponibles dentro de la red), los planes de salud pueden otorgar el estatus de dentro de la red a un proveedor y servicios relacionados. En tales casos, el proveedor acepta la tarifa dentro de la red y el paciente podrá acceder al costo compartido dentro de la red. Puede ser útil contactar al pagador para solicitar que un servicio se convierta en estatus dentro de la red.
- Si el plan lo requiere, ¿se ha obtenido la referencia o autorización previa adecuada? Muchos planes requieren que los servicios no urgentes sean pre-aprobados o que un médico de atención primaria haga la referencia para atención especializada. No obtener las referencias adecuadas o la autorización previa puede resultar en la no remuneración por parte del plan.
APOYO A DECISIONES DE COBERTURA APROPIADAS DEL PAGADOR
Un componente esencial para proporcionar terapias con medicamentos con éxito es trabajar con los pagadores. La mayoría de los pagadores cubrirán terapias con medicamentos médicamente necesarias, pero pueden requerir una justificación clínica más allá de un diagnóstico para establecer la necesidad y la idoneidad del paciente para la terapia. Dichos requisitos pueden detallarse en políticas específicas de medicamentos, como una Determinación Local de Cobertura (LCD) de un Contratista Administrativo de Medicare (MAC) o en la política de beneficios médicos de un pagador comercial, o abordarse a través de un proceso general de autorización previa.
- AUTORIZACIÓN PREVIA
La autorización previa (PA, por sus siglas en inglés) es un proceso de aprobación requerido por el pagador que se utiliza para garantizar que ciertos medicamentos, servicios, procedimientos o sitios de atención sean médicamente necesarios y se utilicen de manera adecuada. Aunque no se aplica a Medicare Original, la PA puede ser requerida por Medicare Advantage y pagadores no pertenecientes a Medicare. Durante el proceso de PA, se exige a los proveedores que presenten evidencia de necesidad médica, que puede incluir:
- el resultado esperado de una terapia prescrita,
- las posibles consecuencias de no utilizar esa terapia, y
- por qué las alternativas no son clínicamente apropiadas.
Una PA adecuadamente respaldada y presentada de manera adecuada generalmente resultará en una decisión de cobertura favorable. Si por alguna razón un paciente no puede cumplir con los requisitos de un pagador para el medicamento que necesita, tiene derecho a solicitar una determinación de cobertura, también conocida como solicitud de excepción.
- SOLICITUD DE EXCEPCIÓN
Una solicitud de excepción es un tipo específico de determinación de cobertura que solicita a un pagador reconsiderar una denegación de cobertura o desviarse del proceso estándar. Ofrece al pagador la oportunidad de influir en el proceso de toma de decisiones de cobertura o hacerlo más específico para el paciente cuando las políticas de cobertura del pagador no satisfacen las necesidades únicas de un paciente. Una solicitud de excepción nuevamente requiere que el médico tratante presente evidencia de necesidad médica. Es útil responder específicamente a las razones por las que se denegó la cobertura (por ejemplo, medicamento no incluido en el formulario, restricciones de dosis, terapia escalonada, etc.).
Una solicitud de excepción que se presente de manera adecuada y esté suficientemente respaldada a menudo resultará en una decisión favorable del pagador. Si la solicitud no se concede, el pagador proporcionará al paciente una explicación por escrito e incluirá información sobre cómo solicitar una apelación.
- APELACIONES
Las apelaciones son una respuesta a la denegación de beneficios por parte de un pagador, beneficios que el afiliado considera que tiene derecho a recibir. El proceso de apelaciones generalmente incluye una serie de pasos progresivos y plazos específicos. Si se respalda una apelación, se debe contactar al pagador para obtener orientación, ya que las políticas individuales pueden variar. Los pasos que los pacientes o proveedores pueden tomar para respaldar una apelación incluyen:
- presentar evidencia de apoyo para contrarrestar la razón específica de la denegación,
- exponer la historia del paciente de manera que conduzca a la solicitud terapéutica (por ejemplo, eventos que llevaron a la condición actual, resultados de terapias previas, progresión clínica esperada, etc.),
- expresar disposición para colaborar (por ejemplo, ofrecer información de contacto, invitar a discutir con un director médico o especialista, etc.).
Tras una decisión de cobertura favorable en cualquier etapa, es importante proporcionar retroalimentación al pagador y reforzar que su decisión resultó en un resultado positivo para el paciente.
FOTOTERAPIA PARA AFECCIONES CUTÁNEAS
La mayoría de las compañías consideran las siguientes intervenciones como médicamente necesarias:
- FOTOTERAPIA UVB DE BANDA ESTRECHA PARA LAS SIGUIENTES INDICACIONES:
- Dermatitis atópica (eccema atópico)
- Urticaria crónica
- Mastocitosis cutánea (después de que las terapias convencionales hayan fallado)
- Linfoma cutáneo de células T
- Micosis fungoide/Síndrome de Sézary en etapas iniciales
- Granuloma anular
- Enfermedad de Kyrle (dermatosis perforante) refractaria a la terapia tópica o intralesional
- Liquen plano
- Morfea (esclerodermia circunscrita)
- Fotodermatosis (por ejemplo, dermatitis actínica y urticaria solar)
- Pitiriasis liquenoide crónica
- Erupción polimorfa lumínica
- Psoriasis
- Prurigo nodular refractario a corticosteroides tópicos o intralesionales
- Prurito urémico refractario a emolientes, analgésicos tópicos, antihistamínicos orales o gabapentina
- Vitíligo
2. UVB CON LA ADICIÓN DE ALQUITRÁN DE HULLA TÓPICO (RÉGIMEN DE GOECKERMAN):
- Para personas con psoriasis severa (definida como psoriasis que afecta más del 10 % de la superficie corporal).
3. TRATAMIENTO DE FOTOTERAPIA DOMICILIARIA (UVB):
- Como equipo médico duradero (DME) para personas con psoriasis severa con antecedentes de exacerbaciones frecuentes que no pueden asistir a terapias en el lugar o que necesitan iniciar terapia de inmediato para suprimir brotes de psoriasis.
- Para personas con dermatitis atópica (eccema) que no pueden asistir a terapias en el lugar.
4. CABINAS DE LUZ ULTRAVIOLETA DOMICILIARIAS O LÁMPARAS UV, ASÍ COMO BOMBILLAS DE REEMPLAZO VENDIDAS SOLO CON RECETA MÉDICA:
- Para personas elegibles para fototerapia UVB domiciliaria.
LAS SIGUIENTES INTERVENCIONES SE CONSIDERAN EXPERIMENTALES E INVESTIGACIONALES, YA QUE NO SE HA ESTABLECIDO SU EFICACIA:
-
- Fototerapia UVB de banda estrecha para todas las indicaciones no incluidas en la lista de intervenciones médicamente necesarias, incluyendo:
- Alopecia mucinosa
- Dermatitis química/dermatitis de contacto
- Colestasis del embarazo
- COVID-19
- Urticaria dermatográfica (también conocida como dermografismo)
- Reacción de hipersensibilidad a medicamentos
- Eritema anular centrífugo
- Máculas/pápulas eritematosas hiperpigmentadas
- Enfermedad injerto contra huésped
- Enfermedad de Grover (dermatosis acantolítica transitoria y persistente)
- Enfermedad de Hailey-Hailey
- Hidradenitis supurativa
- Erupción cutánea por hipersensibilidad
- Amiloidosis liquenoide
- Liquen escleroso
- Liquen simple crónico
- Dermatitis liquenoide
- Papulosis linfomatoide
- Mucinosis papular
- Urticaria papular
- Hipomelanosis macular progresiva
- Prurito
- Esclerodermia
- Hipopigmentación cutánea por cicatrización
- Dermatitis superficial de células mixtas
- Fototerapia UVB de banda estrecha para todas las indicaciones no incluidas en la lista de intervenciones médicamente necesarias, incluyendo:
2.UVB CON LA ADICIÓN DE ALQUITRÁN DE HULLA PARA TODAS LAS INDICACIONES QUE NO SEAN PSORIASIS
- (por ejemplo, pénfigo, prurito);
3. EL USO DE PETROLATO O EMOLIENTES ANTES DE LA RADIACIÓN ULTRAVIOLETA
- Dado que los beneficios clínicos de esta práctica no han sido evaluados en ensayos bien controlados.
4. FOTOTERAPIA DOMICILIARIA (UVB) PARA EL TRATAMIENTO DEL LINFOMA CUTÁNEO DE CÉLULAS T
- (micosis fungoide y síndrome de Sézary) y otras indicaciones distintas a psoriasis y dermatitis atópica (eccema).
5. TRATAMIENTO DOMICILIARIO CON PUVA
- Debido a la insuficiencia de pruebas sobre su seguridad.
TERAPIA DOMICILIARIA
La terapia domiciliaria debe limitarse a UVB y solo es elegible en el hogar cuando el individuo requiere tratamiento UVB al menos tres (3) veces por semana. PUVA no es una opción adecuada para terapia domiciliaria. Oxsoralen es un agente fotosensibilizante potente que solo debe usarse bajo condiciones controladas y bajo la supervisión de un médico.
La fototerapia domiciliaria puede considerarse médicamente necesaria para cualquiera de los siguientes diagnósticos:
- Psoriasis severa; o
- Dermatitis atópica/Eccema severo; o
- Prurito de enfermedad renal; o
- Liquen plano; o
- Micosis fungoide; o
- Pitiriasis liquenoide; o
- Prurito de enfermedad hepática.
La elegibilidad para un dispositivo de terapia domiciliaria depende del cumplimiento de TODOS los siguientes criterios:
- La condición del individuo debe cumplir con uno de los diagnósticos elegibles mencionados anteriormente; y
- Debe haber una respuesta positiva documentada a la luz ultravioleta; y
- Debe ser de naturaleza crónica, requiriendo mantenimiento a largo plazo que exceda los cuatro (4) meses; y
- El dispositivo debe ser solicitado por el médico; y
- El dispositivo debe estar aprobado por la Administración de Alimentos y Medicamentos (FDA); y
- El dispositivo debe ser adecuado para la superficie/cuerpo que se está tratando.
Además de cumplir con los criterios de elegibilidad mencionados, el pago debe limitarse al dispositivo más adecuado que satisfaga las necesidades del individuo. Todas las solicitudes de gabinetes de luz ultravioleta y unidades portátiles se revisarán de manera individual.
La terapia de luz ultravioleta y la terapia domiciliaria que no cumplan con los criterios establecidos en esta política se consideran no médicamente necesarias.
Códigos HCPCS para Fototerapia:
E0691: Sistema de terapia con luz ultravioleta, incluye bombillas/lámparas, temporizador y protección ocular; área de tratamiento de 2 pies cuadrados o menos según lo establecido por CMS, clasificado dentro de los sistemas de terapia con luz ultravioleta.
E1399: Equipo médico duradero (DME), misceláneo. Actualmente se utiliza para facturar DME de bajo costo sujeto a las reglas de 42 C.F.R. 414.220, otros DME cubiertos sujetos a las reglas de 42 C.F.R. 414.229, y partes de repuesto de DME sujetas a las reglas de 42 C.F.R. 414.210(e).

Tratamiento con láser para Psoriasis y otras afecciones cutáneas seleccionadas
La mayoría de las compañías consideran las siguientes intervenciones médicamente necesarias:
- Tratamiento con láser excimer y láser de colorante pulsado para personas con psoriasis en placas localizada de leve a moderada que afecta al 10 % o menos de su área corporal y que no han respondido adecuadamente a 3 o más meses de tratamientos tópicos, incluyendo al menos 3 de los siguientes:
- Antralina;
- Corticosteroides (por ejemplo, ungüento de betametasona dipropionato y crema de fluocinónido);
- Agentes queratolíticos (por ejemplo, ácido láctico, ácido salicílico y urea);
- Retinoides (por ejemplo, tazaroteno);
- Preparaciones a base de alquitrán; y/o
- Derivados de vitamina D (por ejemplo, calcipotrieno);
No más de 13 tratamientos con láser por curso y 3 cursos por año generalmente se consideran médicamente necesarios. Si la persona no responde a un curso inicial de terapia con láser, según lo documentado por una reducción en el puntaje del Índice de Área y Severidad de la Psoriasis (PASI) u otra medición objetiva de respuesta, no se consideran médicamente necesarios cursos adicionales.
2. El uso de láser en acné queloide en la nuca (AKN) para las siguientes indicaciones:
- Excision con láser para el tratamiento de cicatrices extensas observadas en las etapas de placa o tumor del acné queloide en la nuca (AKN), o
- Depilación con láser (remoción de vello con láser) para AKN activa que responde de manera deficiente a la terapia médica (por ejemplo, antibióticos orales y tópicos, y esteroides intralesionales);
La mayoría de las compañías consideran las siguientes intervenciones experimentales e investigacionales debido a la evidencia insuficiente en la literatura revisada por pares y la efectividad de estos enfoques no ha sido establecida:
- Uso combinado de láser de colorante pulsado y ultravioleta B (UVB) para el tratamiento de personas con psoriasis en placas localizada;
- El láser excimer o el láser de colorante pulsado en el tratamiento de formas de psoriasis diferentes a la psoriasis en placas;
- Tratamiento con láser para las siguientes indicaciones (no es una lista completa):
- Dermatitis atópica
- Amiloidosis cutánea
- Heridas cutáneas diabéticas
- Celulitis disecante
- Lesiones eccematosas
- Verrugas faciales (verrugas)
- Granuloma anular
- Granuloma facial
- Herpes simple labial
- Hidradenitis supurativa
- Hidrocistomas
- Infiltración linfocítica de Jessner en la piel
- Queratosis pilaris
- Liquen escleroso
- Lupus eritematoso
- Melasma
- Morfea (esclerodermia de la piel)
- Micosis fungoides
- Xantogranuloma necrobiótico
- Oniquia
- Onicomicosis
- Prúrigo nodular
- Mucinosis eritematosa reticular
- Sarcoidosis
- Dermatitis espongiótica
- Neoplasia intraepitelial vulvar
- Condiciones inflamatorias de la piel vulvar
- Tratamiento ablativo con láser (no contacto, ablación de campo completo y ablación fraccionada) para la cicatrización de heridas.
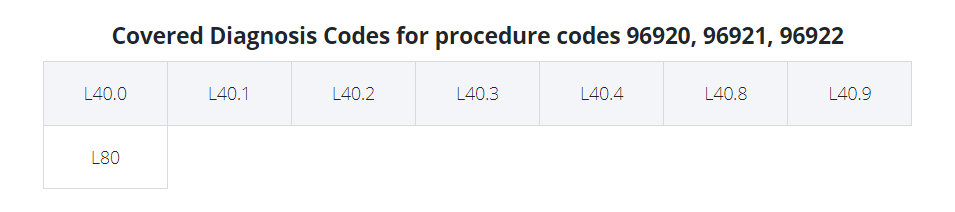
Códigos CPT para Tratamiento con Láser:
- 96920: Tratamiento con láser para enfermedad inflamatoria de la piel (psoriasis, dermatitis atópica, eccema) área total menor a 250 cm²
- 96921: Tratamiento con láser para enfermedad inflamatoria de la piel (psoriasis, dermatitis atópica, eccema) de 250 cm² a 500 cm²
- 96922: Tratamiento con láser para enfermedad inflamatoria de la piel (psoriasis, dermatitis atópica, eccema) más de 500 cm²
Estos códigos técnicamente solo funcionan para psoriasis. Algunos pagadores permitirán su uso para otros diagnósticos (dermatitis atópica, eccema) ya que no existe otro código específico para excímer láser. Si no lo permiten, debe usarse el código 96999 con una descripción escrita adjunta.
Códigos HCPCS (Terapia fototerapéutica en casa (tratamiento UVB)):
- A4633: Bombilla/lámpara de repuesto para sistema de terapia con luz ultravioleta, cada una.
Vitiligo
La mayoría de las compañías consideran los siguientes métodos establecidos como médicamente necesarios para el tratamiento del vitiligo:
- Láser excímer (por ejemplo, XTRAC, PhotoMedex, Radnor, PA; EX-308, Ra Medical Systems, Inc., Carlsbad, CA)
- Ultravioleta B de banda estrecha (NB-UVB)
- Psoralenoterapia tópica y oral (PUVA)
- Tacrolimus tópico
- Corticosteroides tópicos y sistémicos.
La mayoría de las compañías consideran que la continuación de la terapia PUVA o UVB de banda estrecha no es médicamente necesaria a menos que haya una pigmentación folicular significativa después de 6 meses de tratamiento (8 a 10 tratamientos por mes).
La mayoría de las compañías consideran que los siguientes procedimientos son experimentales e investigacionales porque no se ha establecido la efectividad de estos enfoques:
- Las siguientes intervenciones para el tratamiento del vitiligo (no es una lista completa):
- Apremilast (solo o combinado con NB-UVB)
- Injerto autólogo de mini-punching
- Injerto de techo de ampolla (injerto de ampolla epidérmica por succión) (por ejemplo, CelluTome Epidermal Harvesting System)
- Capecitabina
- Láser de dióxido de carbono fraccionado
- Anticuerpo monoclonal quimérico a CD20 (por ejemplo, rituximab)
- Terapia con aguja de fuego
- Glutatión
- Fototerapia en casa
- Interleucinas
- Mesoterapia intradérmica (inyecciones de NCTF135 bio-revitalizant)
- Melagenina
- Hormona estimulante de melanocitos α (por ejemplo, afamelanotida)
- Transplante de melanocitos/cultivo de melanocitos y transferencia de melanocitos queratinocitos no cultivados
- Neovir (un agente inmunomodulador intramuscular, compuesto por oxodihidroacridinilacetato sódico)
- Prostaglandinas (por ejemplo, bimatoprost, latanoprost y prostaglandina E2)
- Injerto de piel de espesor parcial
- Alquitranes
- Minoxidil tópico
- Gel de fenitoína tópico
- Pseudocatalasa tópica
- Agentes de factor de necrosis tumoral-alfa (por ejemplo, adalimumab, etanercept e infliximab)
- Análogos de vitamina D (por ejemplo, calcitriol y paricalcitol).
La mayoría de las compañías consideran los tratamientos para el vitiligo como cosméticos si no afectan la condición subyacente y no resultan en una mejora en la protección contra el cáncer de piel; específicamente, la micropigmentación (tatuaje) y la despigmentación (con monobenziléter de hidroquinona/monobenzona) se consideran cosméticos.
Recursos:
1. https://www.aetna.com/cpb/medical/data/200_299/0205.html

