UVB Phototherapy for Psoriasis
Clinical-grade UVB light therapy solutions designed to support psoriasis treatment in home and clinical settings.
A Smarter Approach to Psoriasis Treatment with UVB Phototherapy
More than 8 million Americans carry a psoriasis diagnosis. A significant portion manage it with topical corticosteroids or vitamin D analogues — effective for limited disease, less so when involvement is extensive or when the skin stops responding to what used to work. At that stage, the question isn’t which cream to switch to.
That’s where psoriasis treatment uvb phototherapy enters the clinical picture. Not as a last option, but as a well-established treatment step that dermatologists have used for decades because it targets what’s actually driving the disease. In psoriasis, the immune system pushes skin cells through their renewal cycle far too quickly — roughly ten times the normal rate. The result is the buildup of plaques, scale, and chronic inflammation patients know all too well.
The same core phototherapy technology supports vitiligo phototherapy, eczema phototherapy, and dermatitis phototherapy, making NB-UVB devices genuinely versatile for households managing multiple skin conditions.
Trusted by clinicians and patients:
- Endorsed by AAD & National Psoriasis Foundation (joint guidelines, 2019)
- Clinical use in dermatology since 1988
- 50+ peer-reviewed trials supporting safety and efficacy
- FDA-cleared devices for home and clinical applications
- Covered by major US insurers — 66+ million Americans now eligible for home phototherapy
- ISO-certified device manufacturing
Trusted & Certified Technology




Why UVB Phototherapy Is Widely Used in Psoriasis Care
 UV light therapy psoriasis specialists have relied on for decades. New medications have come along, but phototherapy is still recommended — because it works differently than any drug, and for many patients, it works better.
UV light therapy psoriasis specialists have relied on for decades. New medications have come along, but phototherapy is still recommended — because it works differently than any drug, and for many patients, it works better.
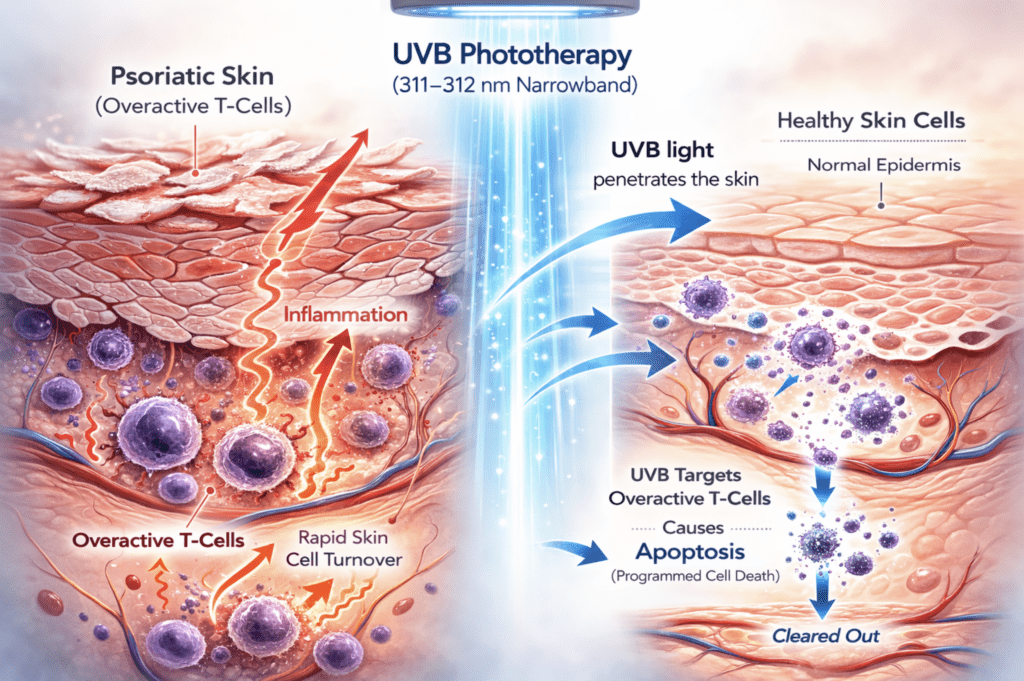
Psoriasis is driven by overactive T-cells that compress the normal 28-day skin renewal cycle to just a few days, causing cells to build up faster than they shed
Creams and ointments work on the surface. UVB light works on the immune cells underneath. At 311–312 nm, narrowband UVB reaches the T-cells inside psoriatic skin and triggers their natural self-destruction — a process called apoptosis. A study in the Journal of Experimental Medicine measured this directly: after one to two weeks of daily NB-UVB sessions, the percentage of T-cells undergoing apoptosis went from 14% to 45%. Healthy skin cells are much less affected — T-cells are about 10 times more sensitive to this effect, which is why the treatment targets the disease and not the surrounding tissue.
As T-cells are cleared out, inflammatory signals drop, cell turnover normalizes, and plaques clear. That’s also why remission after phototherapy can last — the treatment doesn’t just cover up the symptoms, it interrupts the process creating them.
Clinic vs. Home UV Light Therapy: Treatment Pathways Compared
Home uv light therapy psoriasis protocols use the same narrowband technology found in dermatology offices. Both settings use identical technology and both are covered in clinical guidelines. The therapeutic outcome doesn’t change based on where the device is located. What changes is everything around it: scheduling, cost over time, convenience, and realistically, how consistently a patient sticks to the protocol.
A 2024 randomized trial (the LITE study, JAMA Dermatology) ran the comparison across 42 US practices, psoriasis light therapy home device vs office-based UVB, and found no meaningful difference in outcomes. If anything, adherence was better at home, which in phototherapy matters more than most variables.
| Factor | Clinical Setting | Home Setting |
| Clinical supervision | In-person oversight at each visit | Prescribed protocol; remote check-ins as needed |
| Treatment scheduling | Fixed clinic appointments | Self-administered; flexible timing |
| Insurance coverage | Covered by most major insurers with referral; co-pays apply per visit | Many US health plans cover home devices; one-time purchase |
| Sessions to clearance | 20–30 sessions; mean clearance ~58 days at 3×/week | Same protocol |
| Long-term costs | Per-visit costs accumulate across months and years of maintenance | One device investment; lamp replacement after 1,000 hours of use |
| Availability | Tied to clinic location and hours | Usable anywhere |
How to Choose the Right UV Lamp or Clinical System
| Excimer Laser | Handheld Device | Panel Unit | Full-Body Booth | |
| Best for | Localized plaques <10% BSA; scalp; palmoplantar psoriasis | Localized plaques | Generalized psoriasis; nearly whole-body treatment | Generalized psoriasis; whole-body treatment |
| Treatment area | Targeted beam — lesion only, healthy skin unaffected | Spot treatment; repositioned by hand | Nearly full body across a session | Complete body coverage in one session |
| Form factor | Clinical device | Compact, portable | Freestanding panel | Walk-in booth |
| Output / Power | High-intensity targeted beam | Lower irradiance | Higher output than handheld; faster session times | Clinical-grade irradiance; highest output |
Explore UVB Phototherapy Devices & Clinical Systems
Browse the full range of UVB lamps — from portable handheld units to full clinical systems. Both patient-facing and clinical UVTREAT systems are built to that standard.
UVB Phototherapy Devices for Home Use
The argument for psoriasis UVB phototherapy lamps at home isn’t just about convenience. It’s about sustainability. A treatment you can fit around your life is one you’ll actually complete and maintenance sessions become far more realistic when you’re not coordinating clinic availability. The ultraviolet lamp psoriasis treatment relies on the same 311nm Philips medical standard specified in AAD/NPF protocols whether it’s used in a clinic or at home.
Clinical UVB Phototherapy Systems
For dermatology clinics and medical spas, professional-grade UVB systems need to meet a different standard: consistent irradiance across sessions, durable construction for high-frequency use, and output parameters that align with AAD/NPF treatment protocols. UVTREAT clinical systems are built around the same Philips medical lamp platform used in hospital phototherapy units, scaled for clinical throughput.
For localized and treatment-resistant disease, UVTREAT also offers the 308-nm excimer laser — the targeted phototherapy option recommended in AAD/NPF guidelines for palmoplantar psoriasis, scalp involvement, and individual plaques that haven’t responded to whole-body NB-UVB.
How UV Light Therapy Supports Psoriasis Management
Patients may notice reduced itch and plaque softening before visible changes appear at the skin surface. Meaningful visible improvement, where it occurs, typically becomes apparent around weeks 4–6. More substantial changes develop over weeks 8–12 for patients who respond to the treatment.
Studies consistently show that 60–80% of patients who complete a full NB-UVB course achieve PASI-75 – a 75% or greater reduction in psoriasis severity. This holds across skin types: a 2024 systematic review of 54 studies and 1,334 patients with Fitzpatrick skin types III–VI found 70.5% reached that threshold.
UVA vs UVB Phototherapy: Key Clinical Differences
UVA and UVB have decades of clinical evidence and are used in dermatology. But UVA UVB psoriasis therapies operate on different principles and choosing between them isn’t just about efficacy numbers.
Psoriasis narrow band UVB (311–313 nm) Works at the epidermal level without requiring any photosensitizing agent. No psoralen, no drug-light timing window. Suitable for home treatments under physician supervision, recommended as first-line phototherapy by the AAD and NPF. Safe during pregnancy and appropriate for children when topicals have failed. No significant increase in skin cancer risk demonstrated across multiple large retrospective studies. That safety distinction over PUVA is clinically meaningful.
308-nm excimer laser. Both NB-UVB and 308-nm excimer operate within the UVB spectrum, but differ in delivery method, dose distribution, and clinical use. Excimer laser targets individual plaques directly — healthy skin around the lesion gets no exposure at all, it allows much higher doses per session than conventional phototherapy.
PUVA (Psoralen + UVA) Requires oral or topical psoralen administration before each session, making skin significantly more reactive to UVA radiation. Penetrates more deeply — particularly effective for thick resistant plaques, palmoplantar involvement, and cases where NB-UVB hasn’t achieved adequate clearance. PUVA clearance rates can reach 80–90% for severe disease, often with fewer total sessions and longer remission duration. The tradeoff: meaningful cumulative carcinogenic risk. Caucasian patients are generally advised not to exceed ~250 PUVA sessions lifetime. Contraindicated during pregnancy, not suitable for children and cannot be used at home.
In practice: NB-UVB first. PUVA is the escalation path for insufficient response.
Who Can Benefit from Ultraviolet Light Treatments
Ultraviolet psoriasis treatment works across a wide range of patients but whether it’s the right choice for you needs to be discussed with a dermatologist.
Best candidates are people with moderate-to-severe plaque psoriasis that topicals haven’t been able to control, and those who want to stay off systemic immunosuppressants or biologics. Guttate psoriasis tends to respond well and often quickly. Inverse and early erythrodermic psoriasis can be approached with NB-UVB too, though those cases need closer clinical oversight.
Some groups where phototherapy comes up as a particularly useful option: during pregnancy, as nearly all systemic psoriasis treatments are contraindicated or carry significant risk. NB-UVB doesn’t — it’s one of the very few second-line options considered safe in that context. For children where topicals haven’t worked, short courses of NB-UVB are used and generally well-tolerated. Patients with HIV or other conditions that make systemic immunosuppression risky are another group where phototherapy tends to be the preferred option. It also works across all Fitzpatrick skin types — dosing is adjusted accordingly, but efficacy and safety hold from type I through VI.
Before starting, a few things need to be reviewed. Certain conditions: lupus, xeroderma pigmentosum, porphyria affect how skin responds to UV. A history of melanoma, prior ionizing radiation, or arsenic exposure warrants individual risk assessment. Some common medications increase UV sensitivity: tetracyclines, thiazide diuretics, certain NSAIDs and retinoids. Active skin infections or open areas in the treatment zone also need to be resolved first.
Safety Considerations and Treatment Protocols
UVB for psoriasis has a strong long-term safety record and that record is built on using it correctly. Proper dosimetry, protective measures, and medical oversight aren’t just formalities. They’re what makes the treatment work and prevents avoidable side effects.
Dosing. Most protocols start at 70% of the patient’s Minimal Erythema Dose — the lowest UV exposure that produces faint perceptible redness at 24 hours. From there, the dose increases by 10–20% per session as long as no burning occurs. Mild pinkness after a session is the target; it confirms the dose is in the therapeutic range. Actual burning, significant redness, tenderness, blistering means the dose was too high and needs to be pulled back.
Frequency. Three sessions per week is the standard and gets to clearance faster. Two per week is clinically acceptable as well. Daily sessions don’t improve outcomes and increase erythema risk without added benefit. After clearance, once-weekly maintenance sessions are standard for extending remission.
Eye protection. UV-goggles are required for every session without exception. Cumulative unprotected UV exposure to the eyes carries real risk — cataracts and photokeratitis are the primary concerns, and neither is reversible.
Genital shielding. Required for all male patients receiving full-body treatment unless the area itself is being targeted.
Folate. Females of childbearing age are typically advised to supplement folate during a NB-UVB course, as UVB can reduce circulating folate levels.
Monitoring. Erythema response, PASI progression, and cumulative dose should all be tracked throughout treatment. If a burn reaction persists beyond 24–48 hours, or blistering occurs, that warrants dose adjustment and a clinical review — not just waiting it out.
Skin cancer risk. A retrospective study of 3,506 phototherapy patients over a mean of 7.3 years found no significant difference in skin cancer rates compared to the general population.
Light Therapy for Scalp Psoriasis: Special Considerations
The scalp is one of the harder areas to treat with phototherapy, and the reason is straightforward: hair gets in the way. UV light doesn’t penetrate through it, so a standard panel or handheld lamp held near the head isn’t going to reach the skin — the output level doesn’t matter. A UV comb or brush attachment solves this by parting the hair and bringing the lamp into direct contact with the scalp surface.
Expected Results and Treatment Timeline
UVB narrowband psoriasis treatment takes time — and understanding the realistic progression is what keeps patients with a protocol long enough for it to work.
Weeks 1–6: Calibration phase. Doses increment gradually toward the therapeutic threshold. No visible skin changes are expected during this period.
After week 6: For patients who respond to treatment, the first visible changes are reduced scaling, flatter plaques, less itch and they tend to appear no earlier than after 4-6 weeks.
Post-clearance maintenance: Once weekly sessions extend remission substantially compared to stopping treatment entirely. A prospective clinical trial on maintenance NB-UVB confirmed significantly longer time to relapse versus stopping after clearance. Long-term, this is often what makes phototherapy a management strategy rather than a one-time intervention.
NB-UVB Phototherapy vs Biologic Therapy
For patients weighing options beyond topicals, the comparison with biologics comes up regularly.
Efficacy is closer than people tend to assume. NB-UVB reaches PASI-75 in roughly 60–80% of patients who complete a full course. Some biologics — the newer IL-17 and IL-23 inhibitors especially — achieve PASI-90 in a comparable share. The gap is real, though not as wide as it’s often presented.
Cost and safety is very different. Biologic therapy runs $15,000 to $50,000 a year and that’s not a course of treatment, it’s an ongoing commitment with regular injections for as long as it continues. NB-UVB costs a fraction of that over a lifetime of managing psoriasis, involves no medication, and has safety data going back decades. Most biologics haven’t been around long enough to accumulate comparable long-term evidence. On the skin cancer question specifically, NB-UVB has been studied extensively and the answer is reassuring. And for patients who are pregnant, immunocompromised, or dealing with other conditions that rule out systemic drugs — phototherapy is frequently the only option that’s actually available.
Where biologics genuinely pull ahead is speed. Patients on NB-UVB may not see significant clearing until week 8 or later. For someone with severe, widespread involvement who needs results quickly that matters.
One practical point that doesn’t always come up: most US insurers require a documented, adequate trial of phototherapy before they’ll approve biologic therapy.
Medical Disclaimer & Clinical References
This page is for educational purposes only. All phototherapy protocols should be prescribed by a licensed dermatologist. UVTREAT devices are prescription medical devices (21 CFR 801.109).
References used on this page:
- Elmets CA et al. AAD–NPF Joint Guidelines of Care: Phototherapy. JAAD, 2019.
- Gelfand JM et al. Home vs. Office-Based NB-UVB — the LITE Trial. JAMADermatology, 2024;
- Ozawa M et al. 312-nm UVB induces T-cell apoptosis in psoriatic lesions, 1999
- Nakamura et al. NB-UVB in skin of color: systematic review. Photodermatology, Photoimmunology & Photomedicine, 2025.
- LiYet al. UV-based therapy network meta-analysis. Annals of Medicine, 2022.
- Cigna/Anthem Elevance coverage expansion for home NB-UVB phototherapy.Dermatology Times, July 2025.
- Wang, 2024. Retrospective study of 3,506 UVB-treated patients
- National Psoriasis Foundation: psoriasis.org
- American Academy of Dermatology: aad.org
Medical Disclaimer: The information on this page is for educational purposes only and does not constitute medical advice. Always consult a licensed dermatologist before starting UVB phototherapy. Individual results may vary. FDA-cleared devices are indicated for use as directed by a healthcare professional.