Best Pelvic Floor Chair: EMS Chairs for Pelvic Floor Strengthening & Incontinence
In clinical practice, pelvic floor dysfunction presents across almost every patient group, yet it stays underreported. Patients frequently attribute bladder leakage or a sense of pelvic weakness to age or to having given birth, and treat it as inevitable. That assumption is mistaken. The pelvic floor is striated muscle; it adapts to load and deconditions when it is not used, injured, or surgically disrupted. The conditions that most often erode tone and coordination here are childbirth, menopausal change, prolonged intra-abdominal strain, and prostate surgery. What follows clinically is stress, urge, or mixed urinary incontinence.
For many years the standard first response was voluntary contraction training, better known as Kegel exercises. These help a subset of patients, but their success is bound tightly to correct technique and sustained adherence. A non-invasive pelvic floor chair takes a different route, stimulating the musculature directly through a focused electromagnetic field, with no electrodes, no undressing, and no recovery time. The sections below set out how these EMS magnetic stimulation chairs operate, which patients stand to gain from them, how they measure against conventional pelvic floor training, and where two professional KERNEL systems fit in a clinical setting.
What Is a Pelvic Floor Chair and How Does It Work?
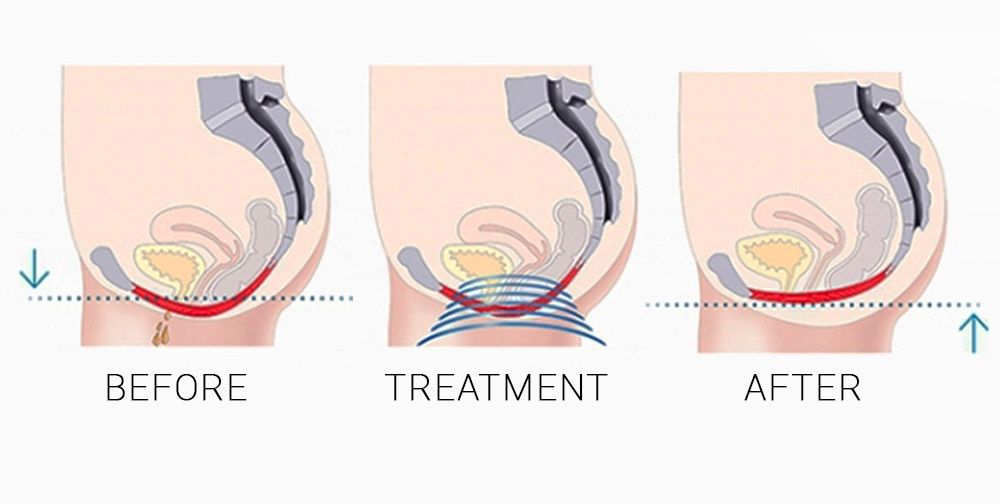
A pelvic chair is a seated unit that applies high-intensity electromagnetic stimulation to the pelvic floor musculature. The patient remains fully clothed and seated while a coil under the seat produces a rapidly alternating magnetic field. By magnetic induction, this field travels through clothing and soft tissue and generates electrical currents; those currents depolarize the motor neurons that govern the pelvic floor, and the muscles contract involuntarily (1). No direct skin contact is required, which is why the same device circulates under several informal names – a magnetic chair for pelvic floor work, a bladder chair, a pelvis chair, or a vaginal chair. The mechanism behind each label is identical. Because the unit reproduces, and automates, the contractions a patient would otherwise attempt by hand, it is also marketed as a kegel chair or a kegel exercises chair.
In the literature the technology appears under more than one heading: High-Intensity Electromagnetic Stimulation (HI-EMT), High-Intensity Focused Electromagnetic technology (HIFEM), functional magnetic stimulation, and extracorporeal magnetic innervation. One property unites them. The evoked contractions are supramaximal – stronger than anything the patient can generate by conscious effort – and they engage fast-twitch and slow-twitch fibers together at a high repetition rate (1). The arithmetic favors the device: a single session delivers a contraction count well beyond what conventional exercise reaches in the same span of time.
That is the real-world gap between this technology and anykegel exercise chair method that depends on voluntary effort. Correct Kegel technique is hard to achieve without guidance. The reported failure rates are high: roughly 30 percent of patients contract the wrong muscles or substitute a Valsalva maneuver (2), and somewhere between 30 and 50 percent of women never perform pelvic floor muscle exercises correctly (3). A pelvic floor ems device takes that variable off the table by contracting the muscles for the patient – and that reliability is much of why these systems now hold a place in pelvic floor rehabilitation, where in physical therapy practices the unit is often referred to simply as a pt chair.
Benefits of EMS Pelvic Floor Chairs
What makes a pelvic floor strengthening chair clinically attractive is the pairing of a measurable muscle response with a comfortable patient experience. The benefits with the most consistent evidence behind them are set out below.
Muscle strengthening. Stimulation that is both involuntary and supramaximal can develop pelvic floor strength more efficiently than voluntary work, particularly in patients whose technique is unreliable. The trial data bear this out. Among postpartum women with stress urinary incontinence studied in a single-blind randomized design, an electromagnetic stimulation protocol yielded significantly greater pelvic floor muscle strength than a Kegel program – 16.5 versus 8.0 cmH₂O (p = 0.006) – even though symptom scores and pad-test results improved in both arms (4).
Urinary incontinence management. Symptom reduction is documented across several studies. In a prospective cohort treated on a magnetic stimulation chair, 47 percent of women with pure stress incontinence and 50 percent with overactive bladder were classified as cured at the two-month mark, while subjective improvement reached roughly 68 to 70 percent (1). A separate randomized multicenter trial set electromagnetic stimulation against pelvic floor muscle training and recorded a markedly larger gain in quality of life for the stimulation group, most of which persisted at twelve months (5).
Postpartum recovery and quality of life. A 2025 systematic review reported gains in both urinary incontinence severity and female sexual function when electromagnetic stimulation was paired with pelvic floor training, with adverse events remaining infrequent, mild, and transient – temporary soreness being the typical complaint (6).
Non-invasive treatment. The most practically significant advantage may be that this functions as a genuinely non invasive pelvic floor exerciser. The patient stays seated and clothed throughout; the sensation is a tingling and a rhythmic pull rather than pain, and nothing about it calls for recovery time afterward.
One qualification belongs here without hedging: outcomes differ according to the patient’s condition, the severity of the dysfunction, and the treatment plan chosen. The evidence is strongest in mild-to-moderate incontinence and in patients who cannot voluntarily isolate the correct muscles. These chairs do not replace surgery in severe pelvic organ prolapse, where comparative data still favor surgical repair on anatomical endpoints (7).
Professional KERNEL Pelvic Floor Magnetic Stimulation Chairs
UVTreat distributes two full-sizepelvic floor chair systems built by KERNEL. Both run on the same treatment principle – non-contact magnetic stimulation reaching up to 5 Tesla of field intensity, 18 built-in clinical protocols, and combined wired-remote and application control – and they diverge on a single technical point that matters for clinical planning.
KERNEL KN-2611M Pelvic Floor Magnetic Stimulation Chair
TheKN-2611M is the wider-range of the two. Its stimulation frequency runs from 0.01 to 60 Hz, so one unit can work both ends of the spectrum: low-frequency settings that calm an overactive bladder or release tense musculature, and higher-frequency settings aimed at strength and endurance. A practice seeing a varied caseload – stress incontinence, urge incontinence, postpartum weakness, pelvic floor pain – can therefore treat several indications from a single chair. It is a floor-standing system built for hospitals, rehabilitation centers, and elder-care settings, with application control handling protocol selection and session tracking.
KERNEL KN-2610M Pelvic Floor Magnetic Stimulation Chair
TheKN-2610M carries the same chassis, field intensity, output, protocol library, and control system as the KN-2611M. The two part company on one specification: its stimulation frequency tops out at 30 Hz rather than 60 Hz, across a 0.01–30 Hz range. Where a clinic’s work concentrates on strengthening and routine incontinence management inside that band, the KN-2610M provides the identical core therapy in a more focused – and usually more accessible – package. As a clinical pelvic floor machine chair it performs the same; the narrower frequency band reflects a tighter treatment scope, nothing more.
Which Pelvic Floor Chair Is Right for Your Clinic?
Selecting the best chair for pelvic floor therapy for a given setting is a question of caseload and treatment goals, not of safety or comfort – on those two counts the KERNEL units are identical.
A higher-volume or multidisciplinary practice – urogynecology, urology, women’s health, or a rehabilitation center handling pelvic pain, overactive bladder, and post-prostatectomy incontinence alike – gains from the wider 60 Hz range of the KN-2611M, since one chair can then be programmed across the full spectrum of presentations. A practice with a tighter focus on pelvic floor strengthening and routine incontinence management may find the KN-2610M the better-matched investment, covering its caseload without paying for capacity it will not use. Space, patient throughput, and budget shape the final call. Because pricing and full regulatory documentation depend on configuration, I would confirm current specifications and reimbursement considerations directly; UVTreat’sReimbursement Guide is a sensible place to start, and the team can be reached throughContact UVTreat.
Comparison of KERNEL Pelvic Floor Chairs
Model
Technology
Best For
Treatment Applications
Clinical Environment
Main Advantages
KERNEL KN-2611M
Magnetic stimulation, up to 5 T, 0.01–60 Hz, 18 protocols
Identical core therapy and safety profile in a tighter, more accessible configuration
Both incontinence chairs run on the same evidence-based principle of supramaximal magnetic stimulation. The value of EMS pelvic floor therapy is that it strengthens muscle patients often cannot train effectively on their own, in a non-invasive format with a strong comfort profile. Which system fits comes down to patient needs, treatment goals, and clinic requirements, and any practice would do well to compare the professional KERNEL systems side by side before committing to a purchase.
A point on regulation, for context. Pelvic floor electromagnetic stimulation chairs sit within an FDA-regulated device category, and the cleared indication language for this class refers to non-invasive stimulation of the pelvic floor musculature to rehabilitate weak muscles and restore neuromuscular control in the treatment of male and female urinary incontinence (8). That clearance attaches to specific devices and models, so the regulatory status of any individual unit should be confirmed before it is relied upon in procurement or marketing.
Share
References
Braga A, et al. Pelvic floor muscle stimulation with a 3-Tesla functional magnetic stimulation chair in women with stress urinary incontinence and overactive bladder. Journal of Clinical Medicine. 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC9145499/
Safety and efficacy of a non-invasive high-intensity focused electromagnetic field (HIFEM) device for treatment of urinary incontinence and enhancement of quality of life. PMC.https://pmc.ncbi.nlm.nih.gov/articles/PMC6851770/
Sacarin C, et al. Chair-based magnetic pelvic floor stimulation and female sexual function in women with urinary incontinence: a systematic review. Journal of Clinical Medicine. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12693354/
Yang X, et al. Effectiveness of extracorporeal magnetic stimulation in the treatment of pelvic floor dysfunction: a systematic review and meta-analysis. Neurourology and Urodynamics. 2025. https://onlinelibrary.wiley.com/doi/10.1002/nau.70082
It is a seated medical device that strengthens the pelvic floor through a focused electromagnetic field. The patient sits clothed while the chair drives the muscle contractions, which is the reason it also goes by magnetic chair for pelvic floor therapy, bladder chair, or pelvis chair (1).
A coil set beneath the seat produces an alternating magnetic field. That field induces electrical currents in the pelvic floor, depolarizes the motor neurons, and drives involuntary supramaximal contractions stronger than voluntary effort can reach (1).
For patients who cannot execute Kegels correctly, it often is - a large share of people recruit the wrong muscles or rely on faulty technique (2,3). In one randomized trial, electromagnetic stimulation produced larger strength gains than a kegel chair therapy program, although symptoms improved under both (4). The sounder framing is as a complement to supervised pelvic floor training rather than an outright replacement for it.
The most-studied groups are women with stress, urge, or mixed incontinence, postpartum patients, and men with post-prostatectomy incontinence (1,6). In men specifically, a clinical trial recorded a significant improvement in symptom scores after a full course of treatment (9).
Yes. The session is done seated and fully clothed - no electrodes, no anesthesia, no downtime. What the patient feels is tingling and a rhythmic contraction, not pain (6).
A frequently cited protocol for this device class runs to about six sessions of roughly 28 to 30 minutes each, spaced around twice weekly over three weeks, then followed by periodic maintenance (5,8). The treating clinician tailors that plan through the chair's built-in protocols, and individual results vary.
Published evidence backs symptom reduction and better quality of life for many patients with mild-to-moderate incontinence (1,5,6). Because the result turns on the underlying cause and the severity, a proper clinical assessment should come before any treatment.
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.