Reflectance Confocal Microscopy for Melanoma: How It Improves Early Skin Cancer Diagnosis
Caught early, melanoma is usually very treatable. An in situ lesion and one that has already reached the dermis behave almost like two different diseases when it comes to outcome. So a skin exam really has one job: spot the lesion that matters, and leave the harmless ones alone. That is harder than it sounds. Plenty of ordinary moles look alarming to the naked eye, and even with a dermatoscope I am often left with spots I cannot call either way. For years the only way to settle it was to cut the lesion out and wait on the pathology report.
Reflectance Confocal Microscopy (RCM) changed that calculation. It lets examine skin down to nearly the cellular level, in a living patient, with no scalpel involved. The sections below address the underlying technology, the mechanism of confocal imaging, the clinical scenarios in which it contributes most to melanoma diagnosis, and its principal limitations.
What Is Reflectance Confocal Microscopy and How Does It Work?
Reflectance confocal microscopy is a non-invasive imaging modality that generates horizontal, gray-scale sections of the skin at a resolution approaching that of conventional histology (6). The technique is also referred to as confocal laser scanning microscopy, and that terminology reflects the optical principles behind it.
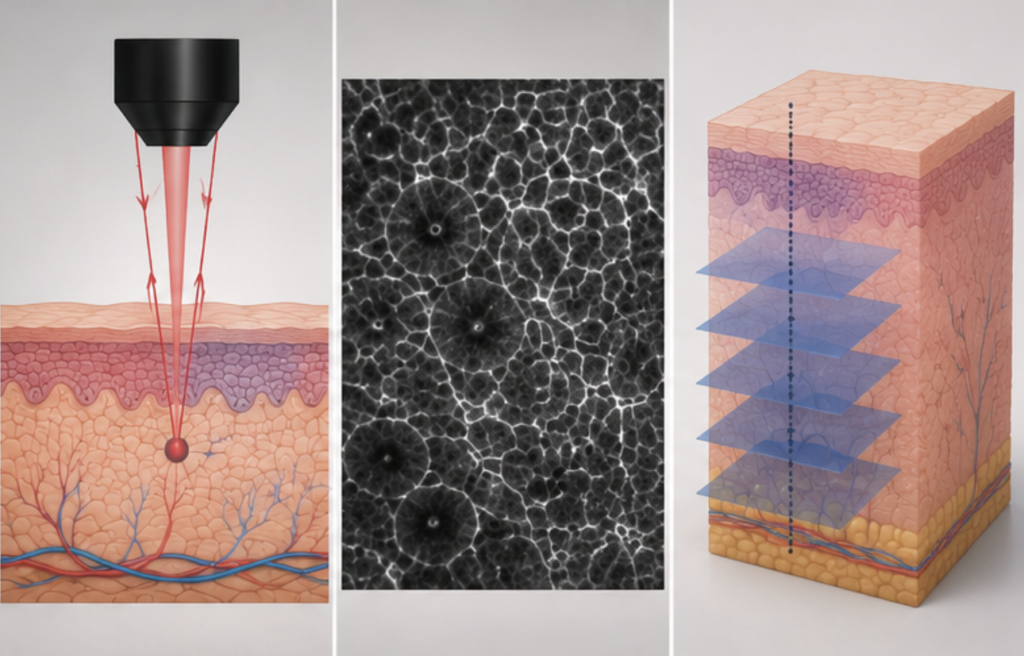
This raises a practical question – what is laser scanning confocal microscopy? A low-power near-infrared laser, operating at 830 nm in commercially available systems, is focused on a discrete point within the skin (10). Reflected light returns through a narrow aperture – the pinhole – before it reaches the detector. This pinhole is the critical element: it excludes any light originating above or below the focal plane, so that only in-focus signal is registered. As the laser scans successively across the plane, the system reconstructs these individual points into a single image. The outcome defines confocal imaging – an optical section acquired at one precise depth, with scattered, out-of-focus light discarded.
RCM does not use dyes or stains. Contrast comes from the tissue itself. Structures with a high refractive index – melanin, keratin, and cellular organelles – reflect more light and appear bright (6). Melanin is a particularly strong natural contrast agent, which is why pigmented cells and melanocytic lesions show up so well. This is a different principle from fluorescence confocal microscopy, which relies on fluorescent labels and is mainly used on excised tissue rather than on a patient’s skin.
In practical terms, a confocal microscope for skin gives lateral resolution of roughly 0.5–1 micron and images down to about 200–250 microns, which covers the epidermis and the papillary dermis (6). The individual field of view is small – around 500 × 500 microns – but the software stitches many frames into a wider mosaic so I can review an area comparable to a dermoscopic view. What I see are individual keratinocytes, melanocytes, dermal papillae, and blood vessels, in real time, in a lesion that is still attached to the patient.
The Role of Confocal Microscopy in Melanoma Diagnosis
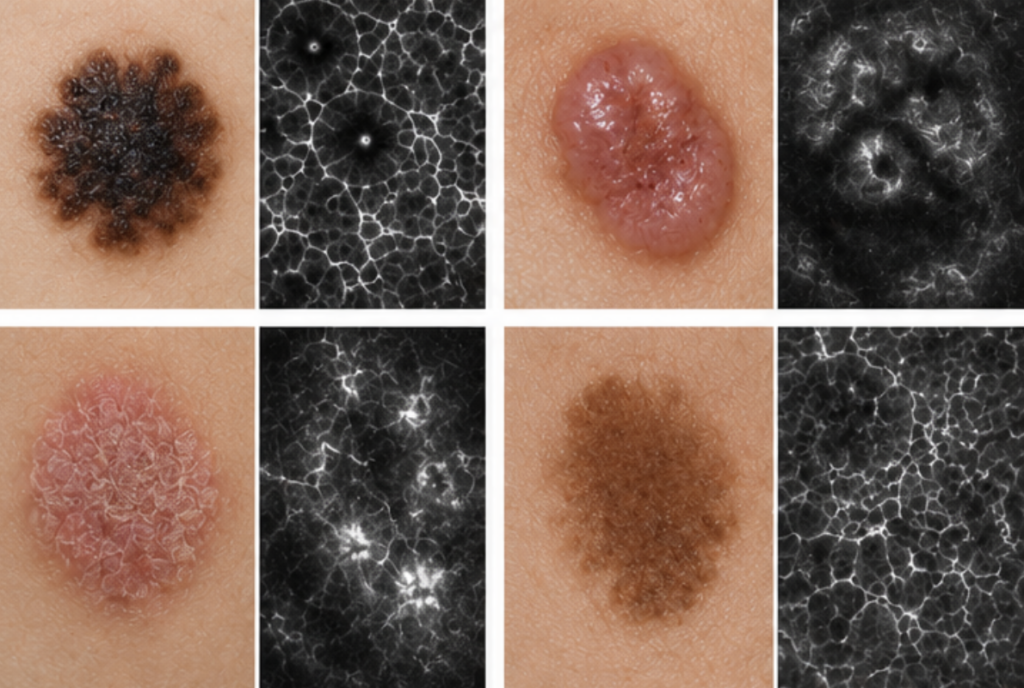
The principal clinical value of reflectance confocal microscopy melanoma assessment lies at the point of decision: a pigmented lesion appears atypical – is a biopsy warranted or not? Dermoscopy is the first-line tool and it is good, but it flags a large number of benign lesions as suspicious. For every melanoma found, somewhere between 5 and 30 benign lesions may be excised, depending on the clinician’s threshold and specialty (1). That means scars, cost, and patient anxiety for lesions that were never dangerous.
Used as a second-level examination on lesions that are equivocal on dermoscopy, RCM improves specificity without sacrificing the ability to catch cancer. The published accuracy figures are consistent on this. A meta-analysis of 32 studies and 7,352 lesions reported pooled sensitivity of 92% and specificity of 70% for melanoma (2). A separate systematic review of clinically equivocal lesions found per-lesion sensitivity of 93% and specificity of 76% (3). A meta-analysis focused on malignant skin tumours reported a melanoma subgroup sensitivity of 92.7% and specificity of 78.3% (4). The exact numbers move with the study design and the lesions selected, but the pattern holds: high sensitivity, and specificity clearly better than dermoscopy alone on hard cases.
The most compelling evidence came from a randomized clinical trial published in JAMA Dermatology in 2022. Pellacani and colleagues enrolled 3,165 patients with suspicious lesions across three Italian centers and randomized them to standard dermoscopic care or standard care plus adjunctive RCM. Applied as a confocal microscope melanoma triage step, the technique reduced unnecessary excisions by 43.4%, while invasive melanomas were still correctly identified at baseline (1). In that trial, RCM was substantially more specific than dermoscopy on equivocal lesions – 82% versus 42% (1). Memorial Sloan Kettering has similarly reported that reflectance confocal microscopy improves melanoma detection while sparing benign lesions from biopsy (10).
This defines the clinical value of confocal microscopy melanoma assessment: fewer benign lesions excised, and very few melanomas overlooked. When a melanoma is confirmed, RCM can also guide where the biopsy should be taken, so the sample is more representative.
Applications of Confocal Microscopy in Dermatology
Melanoma gets most of the attention, but the uses of confocal microscopy extend across dermatology. Broadly there are three types of confocal microscopy relevant to skin: the wide-probe in vivo system for imaging a fixed area of skin, the handheld in vivo probe for curved or awkward sites such as the nose and ears, and the ex vivo system used on freshly excised tissue in the surgical setting.
Basal cell carcinoma is a strong application. A systematic review and meta-analysis of in vivo RCM for primary basal cell carcinoma pooled 15 studies and 4,163 lesions and reported sensitivity of 92% and specificity of 93% (5). RCM can also help subtype BCC and check whether a superficial tumour has cleared after non-surgical treatment. Squamous cell carcinoma and actinic keratosis can be assessed as well, and confocal imaging is useful for tracking response to field therapies such as topical imiquimod or photodynamic therapy, because I can re-image the same area over time without repeated biopsies.
On the face, where biopsies carry a cosmetic penalty, the melanoma microscope proves its worth. Lentigo maligna is notoriously difficult to delineate, and confocal imaging assists both with diagnosis and with mapping the true extent of a lesion before surgery. In the operating context, ex vivo confocal microscopy can examine excised margins during Mohs surgery, giving a rapid read without waiting for frozen or permanent sections.
Application
What confocal imaging adds
Equivocal pigmented lesions
Second-level check that reduces unnecessary biopsies for suspected melanoma
Lentigo maligna
Diagnosis on difficult facial skin and pre-surgical margin mapping
Basal cell carcinoma
High-accuracy diagnosis and subtyping; confirming non-surgical clearance
Actinic keratosis / SCC
Assessment and monitoring of field-directed treatment
Treatment monitoring
Repeatable, scar-free follow-up of the same lesion over time
Amelanotic / hypomelanotic melanoma
An additional tool where dermoscopy is limited by lack of pigment
Table 2. Clinical applications of reflectance confocal microscopy in dermatology.
Benefits and Limitations of Confocal Imaging
RCM is not a replacement for the pathologist, and it is important to be honest about what it cannot do.
The advantages are real. It is non-invasive, so there is no wound and no scar. It works in real time, which means a decision can be made during the visit. It reaches near-cellular resolution and correlates well with horizontal histology, so an experienced reader recognizes familiar structures. Because nothing is removed, the same lesion can be imaged again weeks or months later, which is ideal for monitoring. For patients, that translates into fewer procedures and shorter waits.
The limitations follow from the physics. Confocal microscopy skin only reaches the papillary dermis, roughly 200–250 microns down (6). It cannot see deep tumour or measure Breslow thickness, so it does not stage an invasive melanoma – that still requires excision and histopathology. The field of view is small, so imaging a lesion takes time and patience. Thick, scaly, or ulcerated lesions scatter and block the beam, which degrades the image. And reading RCM well takes training; the learning curve is genuine, and interobserver agreement drops on the most challenging lesions. Equipment cost and limited availability remain practical barriers, though reimbursement has improved access in the United States.
Advantages
Limitations
Non-invasive; no scarring
Imaging depth limited to the papillary dermis
Real-time, same-visit results
Cannot measure Breslow thickness or stage invasion
Near-cellular resolution matching histology
Small field of view; slower per lesion
Repeatable for monitoring
Poor imaging of thick, scaly, or ulcerated lesions
Reduces unnecessary biopsies
Requires trained readers; real learning curve
Table 3. Advantages and limitations of confocal imaging.
This is why I describe RCM as a tool that complements histopathology rather than one that competes with it. It refines the decision about whether to biopsy and where; the microscope slide still confirms the diagnosis and provides staging. Where it fits in the workflow is clear: naked-eye and dermoscopic examination first, RCM on the equivocal cases, and biopsy for anything the imaging cannot reassure me about.
The table below places the three methods side by side.
Feature
Dermoscopy
Reflectance confocal microscopy
Skin biopsy / histopathology
Invasiveness
Non-invasive
Non-invasive
Invasive (tissue removed)
Resolution
Surface and subsurface patterns
Near-cellular (~0.5–1 µm)
Cellular, gold standard
Depth assessed
Surface to superficial
Epidermis to papillary dermis
Full thickness
Result timing
Immediate
Immediate (same visit)
Days (lab processing)
Melanoma specificity on equivocal lesions
Lower (~42%) (1)
Higher (~82%) (1)
Definitive
Main role
First-line screening
Second-level triage of suspicious lesions
Confirmation and staging
Table 1. Confocal microscopy vs dermoscopy vs skin biopsy.
Choosing the Right Confocal Microscope for Clinical Practice
Confocal microscopy in dermatology is not for every clinic. It makes the most sense in settings with a high volume of pigmented lesions and a clinician trained to read the images: academic and referral dermatology centers, dedicated skin cancer and pigmented lesion clinics, Mohs surgery practices, and teledermatology hubs where images can be read remotely. A general practice that sees the occasional atypical mole will get less return than a busy melanoma service.
When evaluating professionaldermatology equipment of this kind, a few specifications matter. Probe type is the first decision – a wide-probe system for flat sites, a handheld probe for curved anatomy, or an ex vivo system for surgical margin work. Beyond that, I look at optical resolution and imaging depth, how well the device integrates with dermoscopy and digital documentation, and the quality of training and support that comes with it. In the United States, one further point is decisive: reimbursement and regulatory status are tied to specific cleared devices, so the equipment has to match the codes it will be billed under. RCM is one of several non-invasive modalities a modern practice may combine, alongside dermoscopy and, for certain non-melanoma cancers, treatment tools such asskin x ray based superficial radiotherapy.
UVTreat works with clinics selecting confocal and other diagnostic imaging systems, and can advise on matching a system to a practice’s caseload, workflow, and regulatory requirements. Choosing well means fewer surprises after installation and a device that earns its place in the clinic.
Reimbursement and Regulatory Note
Since January 1, 2016, RCM of the skin has had Category I CPT reimbursement codes in the United States – 96931 through 96936, covering image acquisition, interpretation, and reporting on a per-lesion basis (7,8). Reimbursement is tied to specific cleared systems, and payment varies by locality. Any device considered for a US practice should be confirmed to be FDA-cleared for the intended clinical use and eligible for these codes before purchase.
Share
References
Pellacani G, Farnetani F, Ciardo S, et al. Effect of Reflectance Confocal Microscopy for Suspect Lesions on Diagnostic Accuracy in Melanoma: A Randomized Clinical Trial. JAMA Dermatology. 2022;158(7):754–761.https://jamanetwork.com/journals/jamadermatology/fullarticle/2792714
Pezzini C, Kaleci S, Chester J, et al. Reflectance confocal microscopy diagnostic accuracy for malignant melanoma in different clinical settings: systematic review and meta-analysis. Journal of the European Academy of Dermatology and Venereology. 2020;34(10):2268–2279.https://onlinelibrary.wiley.com/doi/abs/10.1111/jdv.16248
Stevenson AD, Mickan S, Mallett S, Ayya M. Systematic review of diagnostic accuracy of reflectance confocal microscopy for melanoma diagnosis in patients with clinically equivocal skin lesions. Dermatology Practical & Conceptual. 2013;3(4):19–27.https://pmc.ncbi.nlm.nih.gov/articles/PMC3839827/
Xiong YQ, Ma SJ, Mo Y, et al. A meta-analysis of reflectance confocal microscopy for the diagnosis of malignant skin tumours. Journal of the European Academy of Dermatology and Venereology. 2016;30(8):1295–1302.https://onlinelibrary.wiley.com/doi/abs/10.1111/jdv.13712
Lupu M, Popa IM, Voiculescu VM, Caruntu A, Caruntu C. A Systematic Review and Meta-Analysis of the Accuracy of in Vivo Reflectance Confocal Microscopy for the Diagnosis of Primary Basal Cell Carcinoma. Journal of Clinical Medicine. 2019;8(9):1462.https://pmc.ncbi.nlm.nih.gov/articles/PMC6780971/
Rajadhyaksha M, Marghoob A, Rossi A, Halpern AC, Nehal KS. Reflectance confocal microscopy of skin in vivo: from bench to bedside. Lasers in Surgery and Medicine. 2017;49(1):7–19.https://pmc.ncbi.nlm.nih.gov/articles/PMC5575825/
Centers for Medicare & Medicaid Services. Category I CPT codes 96931–96936: Reflectance confocal microscopy for cellular and subcellular imaging of skin. Effective January 1, 2016.https://www.cms.gov/medicare/physician-fee-schedule/search
FAQ
Dermoscopy magnifies surface and near-surface patterns and is the first-line screening tool. Confocal microscopy images individual cells at greater depth and is used as a second-level check on lesions that remain equivocal after dermoscopy, where it is markedly more specific (1).
Un láser se enfoca en un punto específico de la piel, y un orificio estenopeico bloquea toda la luz reflejada, excepto la que proviene del plano focal. El láser escanea punto por punto para crear una sección óptica, utilizando la melanina y otras estructuras tisulares como contraste natural (6). El dispositivo une múltiples fotogramas para formar un mosaico que se puede revisar.
Sí, para su función prevista. Los análisis combinados reportan una sensibilidad de alrededor del 92-93% y una especificidad de alrededor del 70-78% para el melanoma (2,3,4). Un ensayo aleatorizado encontró que agregar RCM al tratamiento estándar redujo las escisiones innecesarias en un 43,4% sin dejar de detectar melanomas invasivos (1).
No. Solo alcanza la dermis papilar y no puede medir el grosor del tumor ni estadificar un melanoma invasivo (6). Reduce las biopsias innecesarias y orienta sobre dónde tomar la muestra, pero la histopatología sigue siendo el método de referencia para la confirmación y la estadificación.
Melanoma y otras lesiones pigmentadas, carcinoma basocelular, carcinoma espinocelular y queratosis actínica, lentigo maligno y afecciones inflamatorias, además del seguimiento de tratamientos no quirúrgicos (5,9). También se utiliza en tejido recién extirpado para la evaluación de los márgenes quirúrgicos.
La dermatoscopia magnifica los patrones superficiales y subsuperficiales y es la herramienta de cribado de primera línea. La microscopía confocal permite visualizar células individuales a mayor profundidad y se utiliza como método de control de segunda línea en lesiones que permanecen dudosas tras la dermatoscopia, donde resulta notablemente más específica (1).
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.