HomeArticlesWhat Is Photodynamic Therapy? Procedure, Recovery & Common Uses
Written byAnna Chacon,MD; Board-Certified Dermatologist
Published on July 16, 2026
What Is Photodynamic Therapy? Procedure, Recovery & Common Uses
I get asked about photodynamic therapy more often than almost any other in-office procedure I offer, usually by patients who were handed the acronym “PDT” in a referral letter and told very little else. It has earned a steady place in dermatology because it clears sun-damaged skin and some early skin cancers without a scalpel, and the treated area tends to heal cleanly. This guide covers the practical ground: what photodynamic therapy is, how it works inside the skin, the conditions it treats, what the appointment actually feels like, and how recovery and aftercare go. I have kept it to what the clinical evidence supports, and left out the guarantees you sometimes see elsewhere.
What Is Photodynamic Therapy (PDT)?
Here is the photodynamic therapy definition in one line. Photodynamic therapy is a treatment that pairs a light-sensitive drug with a specific wavelength of light to kill abnormal cells (1)(2). If you want to define photodynamic therapy by its parts, “photo” is the light and “dynamic” is the chemical reaction that light sets off once the drug is in place.
So what is PDT treatment, and what does PDT stand for? PDT stands for photodynamic therapy. That is the PDT full form, and it is the same PDT medical abbreviation used in dermatology, oncology and eye medicine alike. When patients ask about the PDT medical meaning, I tell them the name describes the mechanism exactly: light plus a drug that light activates.
Three things have to be present for any of this to happen: a photosensitizing agent, light of the right wavelength, and the oxygen that is already sitting in the tissue (1)(3). Alone, each one is inert. The drug does nothing until light reaches it. The light does nothing to the area until the drug is there to soak it up. That mutual dependence is the whole reason the treatment can be aimed so precisely.
What is photosensitizer, then, and what is a photosensitizing agent in practice? It is a compound that absorbs light and hands that energy to nearby oxygen, kicking off a reaction that damages the cell (1). On the skin we mostly reach for 5-aminolevulinic acid (ALA) or its cousin methyl aminolevulinate (MAL), both painted straight onto the lesion (4)(6). Strictly speaking these are prodrugs. They are not the active photosensitizer until the cell converts them, which is the part worth understanding next.
How Does Photodynamic Therapy Work?
Take it one stage at a time and how photodynamic therapy works stops being mysterious.
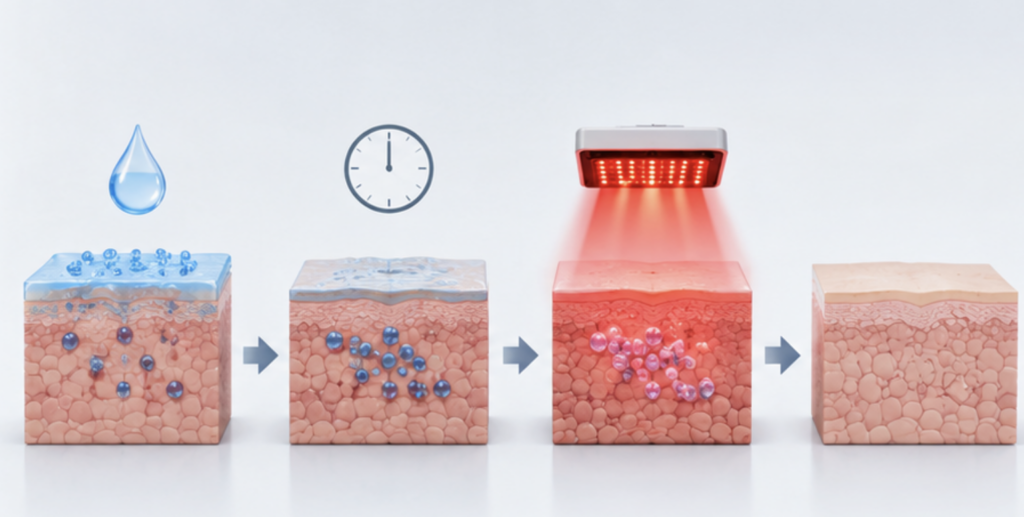
Applying the photosensitizer. We clean the site and apply the photosensitizing agent to the lesion, or across a wider field if the sun damage is spread out. On skin this is a cream, gel or solution (4)(6).
The incubation period. Now the drug sits and absorbs. Inside the cells, ALA and MAL feed into the body’s own heme production pathway and are turned into protoporphyrin IX, and that is the real photosensitizer (1)(3). This is the clever bit. Abnormal, fast-dividing cells, the kind you find in actinic keratosis or a thin skin cancer, soak up the drug and stockpile protoporphyrin IX far more than the calm cells around them, partly because their surface barrier is leaky and their metabolism runs differently (1). That uneven uptake is exactly why the healthy skin next door comes through mostly untouched.
Light activation. Once enough photosensitizer has built up, we shine light of a set wavelength on the area. Blue light near 417 nm and red light near 630 nm are the two workhorses in skin treatment. Red reaches a little deeper, blue tends to be my choice for superficial facial work (1)(4)(6). Under that light the protoporphyrin IX jumps into a high-energy, unstable state. The light source here can be a lamp, a laser or daylight, and it can also be an LED array, which is one reason clinics interested in PDT often already own anLED light therapy unit.
Destruction of the abnormal cells. The excited photosensitizer dumps its energy onto oxygen, generating reactive oxygen species, chiefly singlet oxygen (1)(3). These are short-lived and only act within a whisker of where they form, which is what keeps the damage penned in. They kill the target cells by several routes together: direct oxidative injury, damage to the tiny vessels feeding the lesion, and a local immune response (1)(8). What you are left with is selective destruction of the diseased tissue and relative sparing of the normal skin.
That selectivity is the property everything else hangs on, and it is why PDT belongs to the same broader family of light-based treatments that has drawn so much clinical attention lately.
What Conditions Can Photodynamic Therapy Treat?
Several specialties use PDT, but dermatology is where most patients meet it, and its strongest role is treating precancerous and early cancerous skin lesions. In practice, photodynamic therapy for skin cancer is limited to thin, superficial tumors and the precancerous changes that precede them, not to deep or advanced disease.
The best-evidenced indication is actinic keratosis, the rough scaly patches from years of sun that occasionally turn into skin cancer. Photodynamic therapy for actinic keratosis is FDA approved and in routine use, with complete clearance commonly reported somewhere around 70 to 90 percent depending on the drug and the protocol (4)(6)(9). Its real advantage is field treatment. Because the drug goes on across the whole sun-damaged zone, a single session hits both the lesions you can see and the early ones you cannot yet (9)(10).
Photodynamic therapy for basal cell carcinoma also has a place, specifically for superficial basal cell carcinoma, where topical PDT is an accepted, FDA approved option for certain products (5)(9). I would not use it on thick, nodular or pigmented tumors, and neither would current guidance, because the drug and the light simply cannot reach far enough down. More on that limit further along. PDT is used for Bowen’s disease too, an early squamous cell carcinoma confined to the top layer of skin, where European guidelines support it (9).
Photodynamic therapy for acne is a frequent off-label use. By hitting the oil glands and the bacteria that drive breakouts, PDT can bring down inflammatory lesions, though it is not a first-line choice and protocols are far from standardized (1). When a patient’s acne is stubborn, the decision often comes down to weighing light-based options against systemic drugs, and I walk them through that in more detail in our piece onphototherapy vs biologic treatments. Photorejuvenation of sun-damaged skin is another off-label application.
There are approved uses beyond the skin worth naming in passing, without going deep here. Systemic photosensitizers treat some cases of esophageal cancer, non-small cell lung cancer and high-grade dysplasia in Barrett’s esophagus (7)(8), and a different drug is used in the eye for a form of age-related macular degeneration (11). Same core principle, different agents and different specialists.
Table 1 – Common Conditions Treated with Photodynamic Therapy
Condition
Category
Regulatory status (dermatology, US)
Actinic keratosis
Precancerous skin lesion
FDA-approved
Superficial basal cell carcinoma
Skin cancer
FDA-approved for certain products (5)
Bowen’s disease (SCC in situ)
Early skin cancer
Supported by guidelines; off-label in US (9)
Acne vulgaris
Inflammatory skin condition
Off-label (1)
Photorejuvenation / sun damage
Cosmetic / actinic damage
Off-label (1)
Esophageal / lung cancer, Barrett’s dysplasia
Oncology (non-skin)
FDA-approved, different agent (7)(8)
Wet age-related macular degeneration
Ophthalmology
FDA-approved, different agent (11)
Photodynamic Therapy Procedure: What to Expect
The exact photodynamic therapy procedure shifts with the diagnosis and the product, but the shape of the visit stays the same.
Preparation. On the day, I clean the skin and often scrape off surface scale or crust with light curettage, or wipe the area with a degreasing agent, so the drug soaks in evenly (6)(9). Patients are usually told to keep out of strong sun in the days before.
Applying the photosensitizer. The ALA or MAL goes onto the treatment area. Some protocols then cover it to push absorption along (6).
Incubation. This is where most of the clock goes. The drug has to sit long enough to convert into protoporphyrin IX, which runs anywhere from about an hour to three hours, sometimes under occlusion, depending on the product (4)(6). Daylight PDT flips this around: a short wait, then roughly two hours outside in natural daylight instead of under a lamp (9).
Light exposure. Then comes the light. Conventional blue-light treatment for actinic keratosis usually runs a little over 16 minutes of continuous exposure, and red-light protocols keep their own timing (4)(6). Everyone in the room wears eye protection while the lamp is on.
Add it up and, because incubation dominates, a full visit often eats two to four hours even though the light part is brief.
Does it hurt? That is always the first question. Application and incubation are comfortable. The light phase is the sticking point, and it can bring a burning, stinging or prickling feeling in the treated skin, which is the complaint I hear most (1)(6). A fan, cool air or short pauses usually keep it tolerable, and it stops the moment the lamp goes off. Daylight PDT is far gentler and is a big reason it has caught on for widespread sun damage (9). Straight after, the skin looks red and feels warm, much like a sunburn. How many sessions you need depends on the diagnosis. Actinic keratosis and superficial skin cancers often take one or two, sometimes a few weeks apart, and I confirm the plan case by case.
Recovery, Aftercare, Benefits, and Possible Side Effects
Recovery and healing
Photodynamic therapy recovery is usually uncomplicated. For a day or two the skin is red, puffy and tender, and over the next several days it crusts, flakes and peels as the damaged cells shed (1)(6). Most people settle in one to two weeks, though photodynamic therapy recovery time depends on how large an area was treated and what for. Fresh skin comes in behind the old.
Aftercare
The one rule that matters most in photodynamic therapy aftercare is light protection. Active photosensitizer lingers in the skin for a while after the session, so strong sun or bright indoor light in roughly the first 48 hours can set off an exaggerated phototoxic reaction, essentially a bad sunburn (4)(6). I tell patients to plan on staying indoors and away from windows for about two days, and to cover up with a wide-brimmed hat and clothing when they do go out. Ordinary sunscreen will not save you here, because it does not block the visible light that switches the drug on. Physical cover does. After that, gentle cleansing, a bland moisturizer and leaving the crusts alone are about all that is needed.
Benefits
The photodynamic therapy benefits are the reason it has held on in dermatology. It is non-invasive, with no cutting and nothing to stitch, so there is no surgical wound. Cosmetic results are usually good, often without the scar surgery can leave (9). It treats a whole field of sun damage at once, catching early lesions before they surface (9)(10). It can be repeated on the same area if you need to. And it concentrates the damage on abnormal cells while leaving healthy tissue largely alone.
Limitations
Against that, the honest limits. PDT does not penetrate deeply, so it is wrong for thick, nodular, deeply invasive or pigmented tumors, which either sit too deep or absorb the light before it does any good (5)(9). The discomfort under the lamp puts some patients off conventional PDT. Treatment can mean more than one long visit. And results for certain tumors are less reliable than surgery. It is not for everyone, either: PDT is off the table in porphyria, in a known allergy to the photosensitizer or its ingredients, and in some photosensitivity disorders (4)(6). Special populations need their own judgment call, and for younger patients I would point colleagues to our notes onphototherapy for pediatric dermatology before proceeding.
Table 2 – Benefits vs Possible Side Effects of Photodynamic Therapy
Benefits
Possible side effects
Non-invasive, no surgical wound
Redness (erythema) and swelling (1)
Good cosmetic healing (9)
Burning or stinging during light exposure (1)(6)
Treats a whole sun-damaged field (9)
Crusting, scaling and peeling while it heals (1)
Repeatable on the same area
Temporary shifts in skin pigment (1)
Spares healthy surrounding tissue
Raised light sensitivity for about 48 hours (4)(6)
Avoids scarring seen with some surgery
Rarely, infection or scarring (1)
Nearly all the photodynamic therapy side effects above are temporary, part of the skin healing rather than a complication. Going over them plainly before we start is, in my experience, what keeps patients satisfied afterward, because nothing that happens catches them off guard.
Summary
Photodynamic therapy puts three things together, a light-sensitive drug, light of a specific wavelength and the oxygen already in your tissue, to destroy abnormal cells while mostly sparing the skin around them (1)(3). It is best established for actinic keratosis, with recognized roles in superficial basal cell carcinoma and Bowen’s disease, and off-label use for acne and photorejuvenation, plus separate approved uses outside dermatology (4)(5)(9). The procedure avoids surgery, recovery is generally a week or two of redness and peeling, and the cardinal aftercare rule is keeping the skin out of bright light for about two days. Tissue selectivity, field treatment and clean cosmetic results are what make it such a useful non-surgical option.
Results, though, ride on patient selection, careful drug application and reliable light delivery, which is where equipment quality shows. UVTreat supplies professional PDT and light-based systems, from clinicaldermatology equipment and calibratedinfrared light panel units to full-bodyLED lights bed systems built for consistent, repeatable treatment. If you are standing up an in-clinic PDT service or widening an existing light-therapy offering, dependable hardware is what turns the evidence above into results you can trust.
U.S. Food and Drug Administration. Levulan Kerastick (aminolevulinic acid HCl) for topical solution – Prescribing Information.
U.S. Food and Drug Administration. Ameluz (aminolevulinic acid hydrochloride) gel, 10% – Prescribing Information.
U.S. Food and Drug Administration. Metvixia (methyl aminolevulinate) cream – Prescribing Information.
U.S. Food and Drug Administration. Photofrin (porfimer sodium) for injection – Prescribing Information.
National Cancer Institute. Photodynamic Therapy for Cancer – patient and clinician information.https://www.cancer.gov
Morton CA, Szeimies RM, Basset-Séguin N, et al. European Dermatology Forum guidelines on topical photodynamic therapy. Journal of the European Academy of Dermatology and Venereology.
Eisen DB, Asgari MM, Bennett DD, et al. Guidelines of care for the management of actinic keratosis. Journal of the American Academy of Dermatology; American Academy of Dermatology.
U.S. Food and Drug Administration. Visudyne (verteporfin for injection) – Prescribing Information.
Strong sunlight and bright indoor light for roughly 48 hours, since the skin stays very light-sensitive and can burn badly. Don't pick at crusts, and rely on clothing and a hat rather than sunscreen alone (4)(6).
PDT significa terapia fotodinámica. "Foto" es la luz, "dinámica" es la reacción química que la luz desencadena una vez que se aplica el fármaco (1).
Se aplica un fármaco fotosensibilizador que es absorbido por las células anormales, donde se convierte en un fotosensibilizador activo. Luego, la luz de la longitud de onda adecuada hace que reaccione con el oxígeno, produciendo moléculas reactivas que destruyen las células objetivo (1)(3).
Un compuesto que absorbe la luz y transfiere la energía al oxígeno, creando moléculas reactivas que dañan las células. En la piel, el ALA y el MAL se convierten dentro de las células en el fotosensibilizador activo, la protoporfirina IX (1).
Principalmente queratosis actínica, carcinoma basocelular superficial y enfermedad de Bowen, además de acné no autorizado y fotorejuvenecimiento. Fuera de la piel, los tratamientos relacionados abordan algunos cánceres de esófago y pulmón y una forma de degeneración macular (4)(5)(7)(9)(11).
Resulta cómodo durante la aplicación, pero la fase de luz puede causar quemaduras, escozor o picazón. Esto desaparece al apagar la lámpara, y la terapia fotodinámica con luz diurna provoca una incomodidad notablemente menor (1)(6)(9).
La luz en sí es corta, a menudo un poco más de 16 minutos para el tratamiento con luz azul, pero la incubación del medicamento agrega de una a tres horas, por lo que una visita completa suele durar de dos a cuatro horas (4)(6).
Enrojecimiento, hinchazón, ardor durante el tratamiento, formación de costras, descamación, pelado y cambios de pigmentación transitorios, junto con una mayor sensibilidad a la luz durante aproximadamente dos días (1)(4)(6).
La mayoría de las personas se recuperan en una o dos semanas a medida que el enrojecimiento disminuye y la piel se descama y se renueva, dependiendo del área y la condición (1)(6).
Exposición intensa al sol y a la luz brillante en interiores durante aproximadamente 48 horas, ya que la piel permanece muy sensible a la luz y puede quemarse gravemente. No se rasque las costras y utilice ropa y un sombrero en lugar de solo protector solar (4)(6).
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.